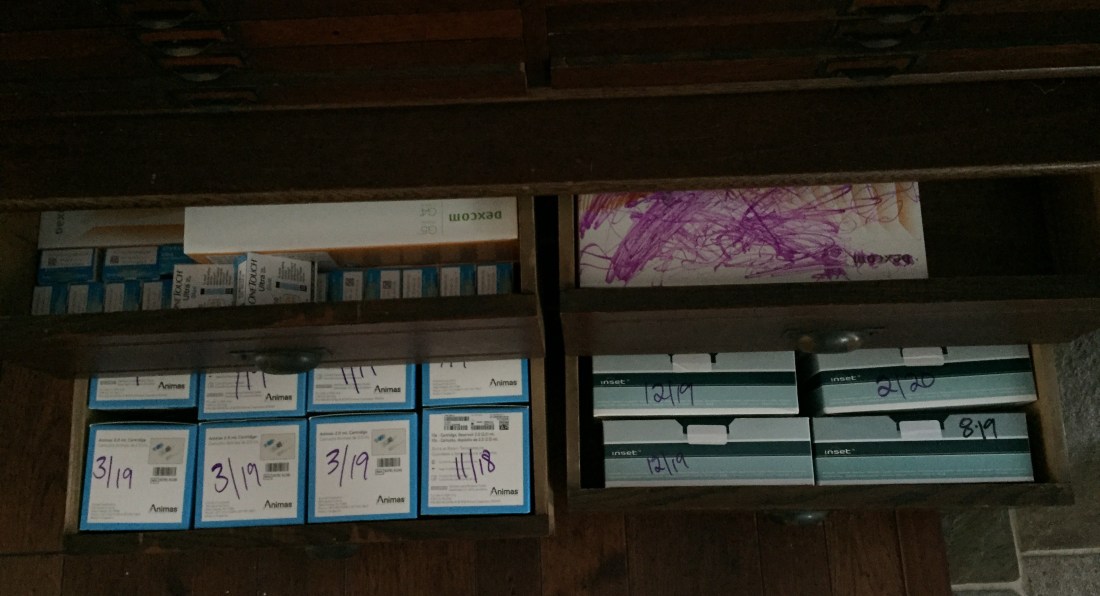
So when we end up in uncomfortable situations, sometimes we end up saying things we wouldn’t normally say, or maybe even things we don’t really mean. Sometimes we stop listening and as a defense mechanism just try to shut the conversation down. Most times the other person is just looking for someone to listen to them and maybe they are asking you to listen because you are important to them, what they are saying is important to them, OR you just happened to be there when they decide to share it. We have all been there; we have all been the person looking to share and also the person receiving information. Sometimes the information is hard to follow, sometimes it is hard to hear, and sometimes it is hard to give. What really matters though is that we listen. So where am I going with this? In the T1D community we all share with each other the worst things that have been said to us about our disease. Most of the time, these things are said just when we are stating that we have the disease. Sometimes the conversation can start because someone sees our insulin pump or pump site, or they see us checking our BG, or shoving some sort of food in our mouth quickly, or as most of you know I have a medical ID tattoo and sometimes people notice that too. So I have asked some friends if they would share some of the things said to them. Here is goes…“If you just ate healthier it would go away. If you eat healthy and exercise you are cured right? You can only have that if you are a kid right? Are you contagious? If you believed enough you wouldn’t have it. You still have it because deep down you don’t not want it to go away enough. I think you are meant to have it for some reason in life. God wouldn’t give you what you can’t handle. If you believed in Jesus enough you wouldn’t have this disease. Stop being selfish and just eat what everyone else made for you. I made this for you gluten free so you can eat it. I made this for you low calorie so you can eat it. I make this for you low fat so you can eat it. I made this for you so you need to eat it. Do you need to check your blood sugar in front of me? Can’t you inject your insulin in the bathroom, it makes people uncomfortable. It is all just in your head. Can’t you just suck it up? You aren’t going to just die are you? Oh, you should stop eating doughnuts.”
Ok, so I am going to stop there because I could go on, but I feel like you all now get the point. First I want you to now think about someone that has an ailment that is visual, such as a leg amputation, (which can be one of the complications of T1D), and reread those comments leaving out the diabetes specific ones of course. Again a dynamic shift right? With T1D being an “invisible” disease, meaning unless you see a pump on our arm, you can’t physically tell we have the disease, for some reason people feel much more comfortable saying extremely rude things. Keep in mind NON OF THIS IS OK TO SAY TO ANYONE! This goes for any disease or bodily difference, if you don’t know what to say, don’t say anything at all. If you are curious, most of us don’t mind if you just ask us but start the conversation with an actual question and not an assumption. For instance, what is it like having T1D? Or I am not quite sure what T1D is do you mind telling me? Also a very sweet friend told me last night, that although she didn’t understand because she didn’t have the disease she could give me empathy because that is what she is good at. That meant so much to me. That is what we all want as humans is understanding, for some one to listen. This day and age makes it very easy for us to preach and not listen. That is how we got where we are. That is where anger breeds, is in misunderstanding. Sure I can be angry about what people say to me, but most of it comes from fear and a lack of understanding. Instead, I choose to educate. It takes bravery to ask questions and really, REALLY pay attention to what is going on around us. To learn about the people we are around everyday. Most of the time I find that once you get through the initial awkwardness and misunderstanding people are just curious and want to learn. We all have minds that want to learn and grow. I never expect everyone to know all about T1D, because our brains simply aren’t made to know everything and unless they have personal experience with the disease it is a lot of information to retain in you brain. I do expect though that people treat me, as they would want to be treated and so that is why I do the same.